by Matthew Lampa, OD

Introduction:
Myopia is core and central to the daily life of the eye care practitioner and the world eye care community has focused much of its research attention on myopia and its progression. Considerable research has supported the role of the peripheral retina and correction of peripheral optics in the control of myopia. This is such an exciting topic in optometry and specifically in the area of contact lenses as the optical profile left behind in the post-orthokeratology cornea is thought to be what is responsible for the lack of progression of myopia in those children who undergo the procedure. This optical profile can also be mimicked with soft center distance multifocal contact lenses. Studies have supported the usefulness of these contact lenses, both orthokeratology and soft center distance multifocal contact lenses, in the area of myopia control.
In asking ourselves as eye care practitioners how to best deliver these complex optics to the patient it is useful to analyze what is in the myopia literature that provide us clues into what the optimum optical profile may be. Once we understand the importance of the optics we can then begin to design and prescribe contact lenses to best meet the needs of our patients.
What We’ve Learned from Orthokeratology:
As stated earlier, so much of what we have learned in the control of progression of myopia in the last several years we have learned through orthokeratology prospective studies. For the management of myopia utilizing orthokeratology the goal is to transform the patient’s corneal epithelium into a lens that first of all fully corrects their nearsightedness centrally. In other words we want to optimally place the central image on the patient’s fovea. This results in optimal central acuity.
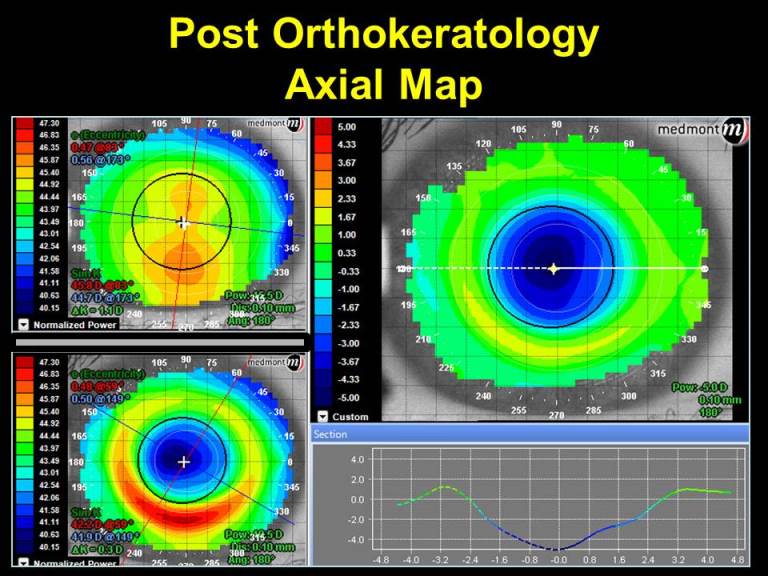
Next, moving out from center, the topographical findings we come across are that of a small central optic zone and a smooth gradual change in power that begins at the periphery of the small central optic zone to the end of the treatment zone or topographical optic zone. Reference the post orthokeratology topography map in Image A below. The small central optic zone on difference display (right image) identifies approximately 4.50 D of central flattening (-4.50 D correction of myopia) and gradually increases in power reaching 4.50 D of relative steepening (+4.50 D add power) at the end of the treatment zone at a cord length of 5mm.
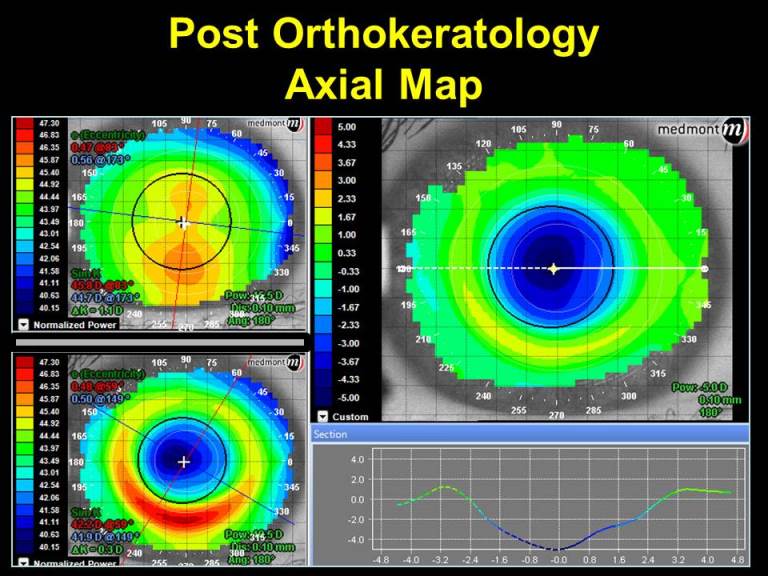
(Image A)
Due to the conservation of corneal power, it cannot be created or destroyed in orthokeratology it can only be redistributed. This means that the power at the end of the treatment zone is equal and opposite to the amount of myopic correction at the center. For example, if after successful orthokeratology a patient has 3.00 D of central flattening (treating -3.00 D of myopia) the amount of power at the end of the treatment zone (topographical optic zone) will effectively be a +3.00 D (analogous to a +3.00 D add).
Distance Center Soft Multifocal Contact Lens Optics & Myopia Control:
As the optics of a traditional soft multifocal contact lens are placed on the front of the contact lens this becomes optically accessible to us when wanting to see where and by how much the power of a soft multifocal contact lens is acting on the patient.
By first performing corneal topography of the patient without contact lenses (bare/natural cornea) this serves as a baseline by which later corneal topography images can be compared. Once the baseline corneal topography is completed images can be taken over the top of center distance multifocal soft contact lenses and then viewed in difference display mode.
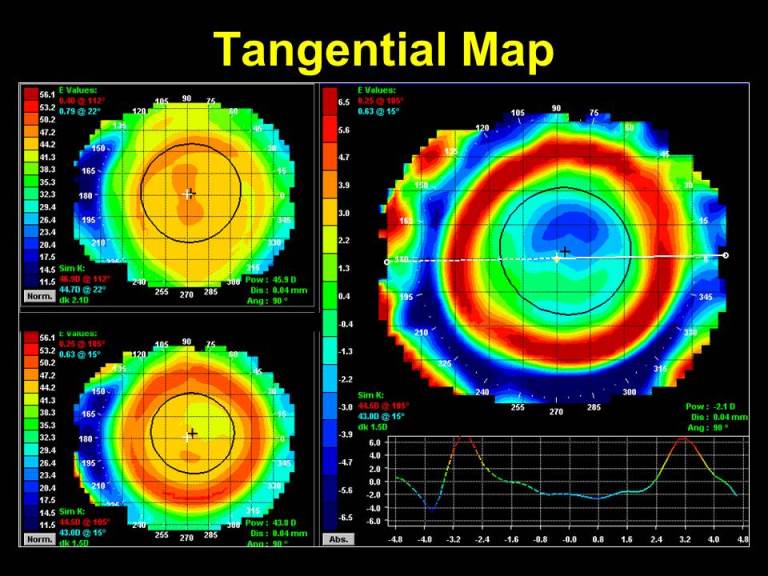
Viewing the tangential maps utilizing the difference display can assist us in indicating position. It lets us know where the contact lens and its subsequent power are placed on the patient’s eye. Below, reference Image B for an example. The map on the top left is topography taken over the bare cornea. The map on the bottom left is topography taken over a distance center multifocal contact lens. The larger map to the right is the difference of the two maps and is a representation of the multifocal optics. It is important to remember that the center of the topography map is the patient’s line of sight and not the geometric center of their eye. By performing corneal topography over the contact lens you take into account the power of the contact lens, how it is positioning/fitting on their eye and how these relate to the patient’s line of sight.
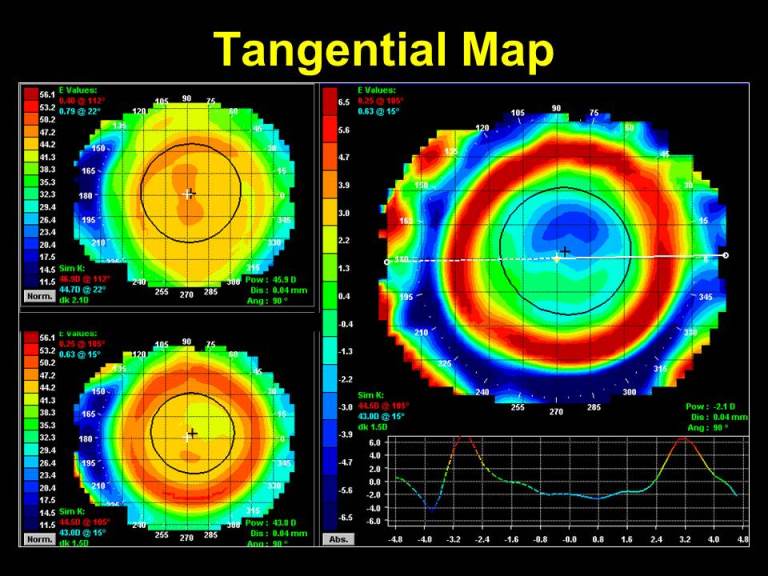
(Image B: Tangential display provides a smoothing of the shape profile and attempts to compare how one point of curvature relates to another or how the slope or shape changes across the cornea.)
By mimicking the optical profile found in post-orthokeratology in a center distance soft multifocal contact lens we can attempt to take advantage of the optic that is thought to be responsible for the control of myopia. When using a custom soft multifocal, not only can the central distance power and surrounding near add power be specified, but the size of the zones housing these complex optics can also be varied (see images D & E below).
SpecialEyes has a unique product line that offers 2 different custom soft multifocal contact lenses – the 54 Bifocal and 54 Multifocal.
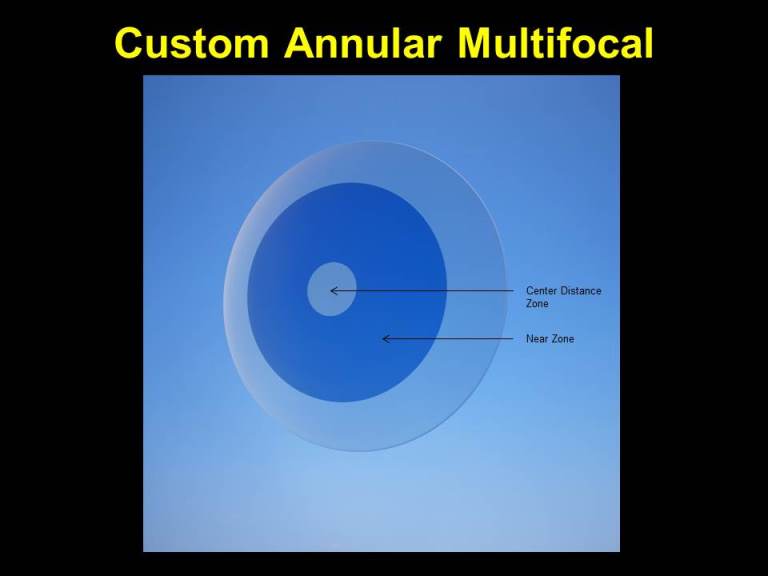
The 54 Bifocal is a simultaneous annular two-zone design and is available in a center distance design. The add power, sphere power, cylinder power, and size of the center distance zone are all customizable. As an example, we as practitioners could design a -3.00 distance center bifocal contact lens with a +2.50 add and 2.0mm center distance zone. The 2.0mm center distance zone would contain full distance power and adjacent to that zone would be an annular zone that comprises full near power. In this initial design, if your young patient experiences too much blur that disturbs their central acuity, you could modify the design to address that. You would either increase the size of the distance center zone or decrease the add power to help increase patient adaptability and decrease the disturbing blur. This design is depicted in Image D below.
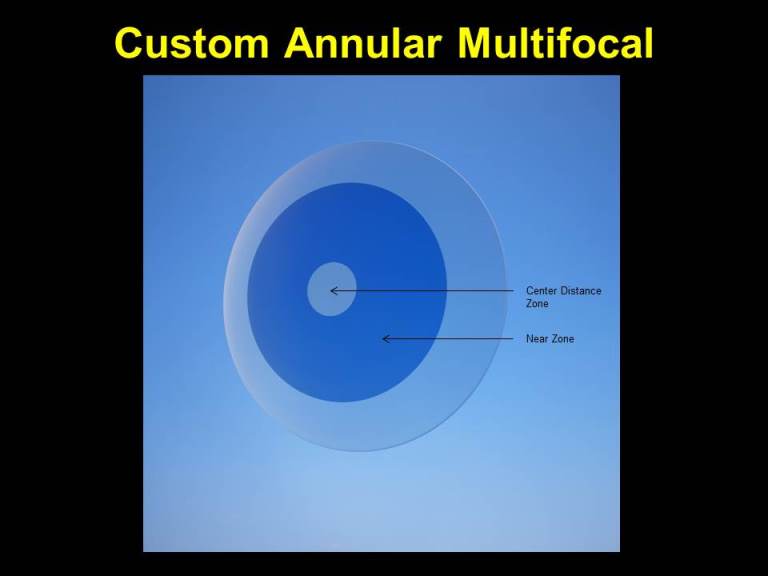
(Image D: Graphical representation of the SpecialEyes 54 Bifocal)
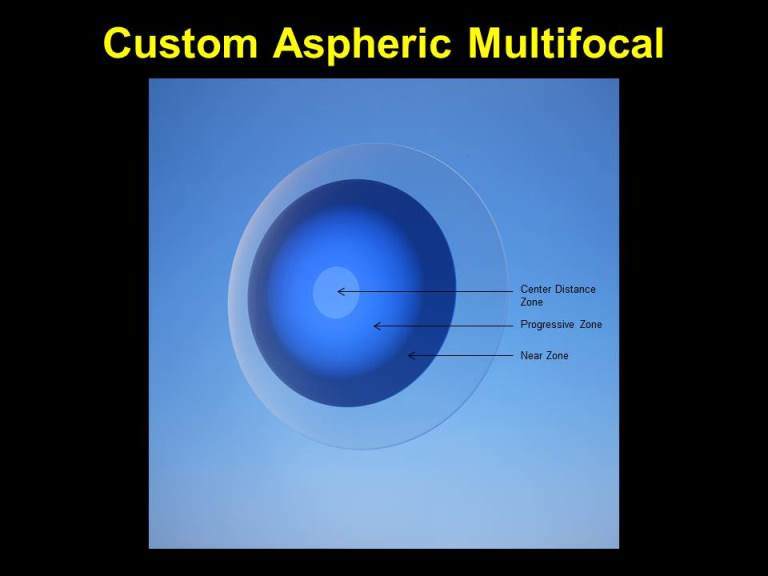
The 54 Multifocal is SpecialEyes’ custom aspheric multifocal contact lens design. This lens is available in a center distance design as well. In this design, the power slowly transitions or progresses from full distance power in the center of the lens to full near power in the periphery of the lens, which is what differentiates it from the 54 Bifocal. The add power, sphere power, cylinder power, size of the distance center zone, and the point at which we reach full near power in the periphery are all customizable. As practitioners, we have control over how fast we would like to transition to full near power and we have control over the size of the center distance zone as well. This design is depicted in Image E below.
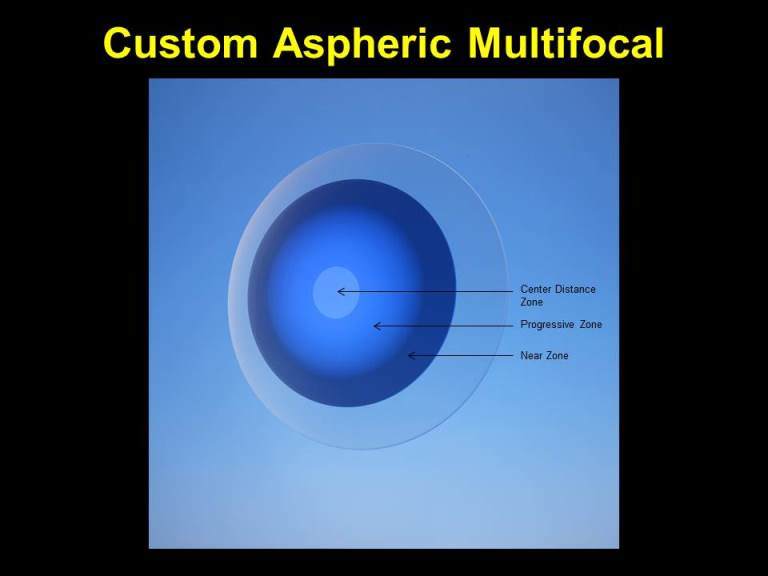
(Image E: Graphical representation of the SpecialEyes 54 Multifocal, center distance design)
In conclusion, using your corneal topographer and a little innovation, custom soft multifocal contact lenses can take on a whole new meaning in practice and help to provide unique care to our younger patients.
Matthew Lampa, OD, FAAO
Dr. Lampa is an Associate Professor of Optometry at Pacific University and a consulting optometrist to SpecialEyes.