A misalignment between the multifocal optics and visual axis can occur due to a variety or combination of factors. Let’s take a look at some of these factors in closer detail.
Scleral Shape
In an average eye, the nasal portion of the scleral is usually more elevated than the other quadrants of the eye1 (Figure 1). This may explain the commonly observed temporal decentration of soft contact lenses, especially in cases of large diameter soft lenses. This in turn, impacts the position of the lens optics. Since multifocal contact lenses rely on complex optical delivery system, even a minimal amount of lens decentration, which can be difficult to see via slit lamp, can lead to vision issues associated with a misalignment between the center of the multifocal optics and visual axis.
Figure 1. The nasal portion of the sclera is usually more elevated which can contribute to commonly observed temporal decentration of soft contact lenses.
Pupil Decentration
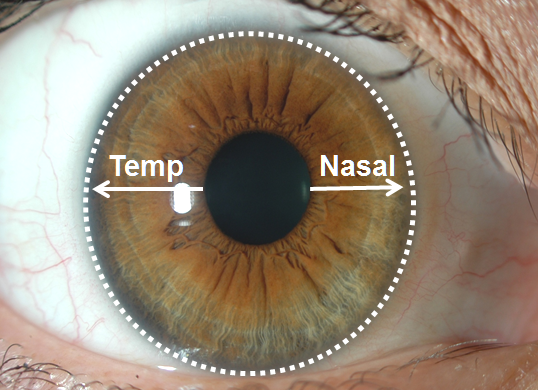
Research has shown that the pupil position within the iris may be another anatomical feature that contributes to a misalignment between the center of the multifocal optics and the visual axis. In a study conducted by Pacific University, it was found that most patients’ pupils are decentered in the superior and nasal direction (Figure 2). This decentration becomes even more pronounced as the pupils become smaller. Additionally, it is important to keep in mind that the visual axis is positioned nasally to the center of the pupil. When we combine these issues, it can be problematic for patients wearing multifocal contact lenses, especially if the lens itself decenters temporally.
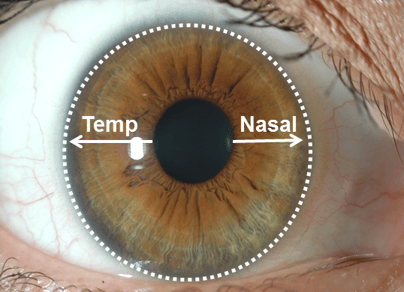
Figure 2. The pupil is not located in the center of the cornea, but rather slightly nasal.
The Fovea & Angle Kappa
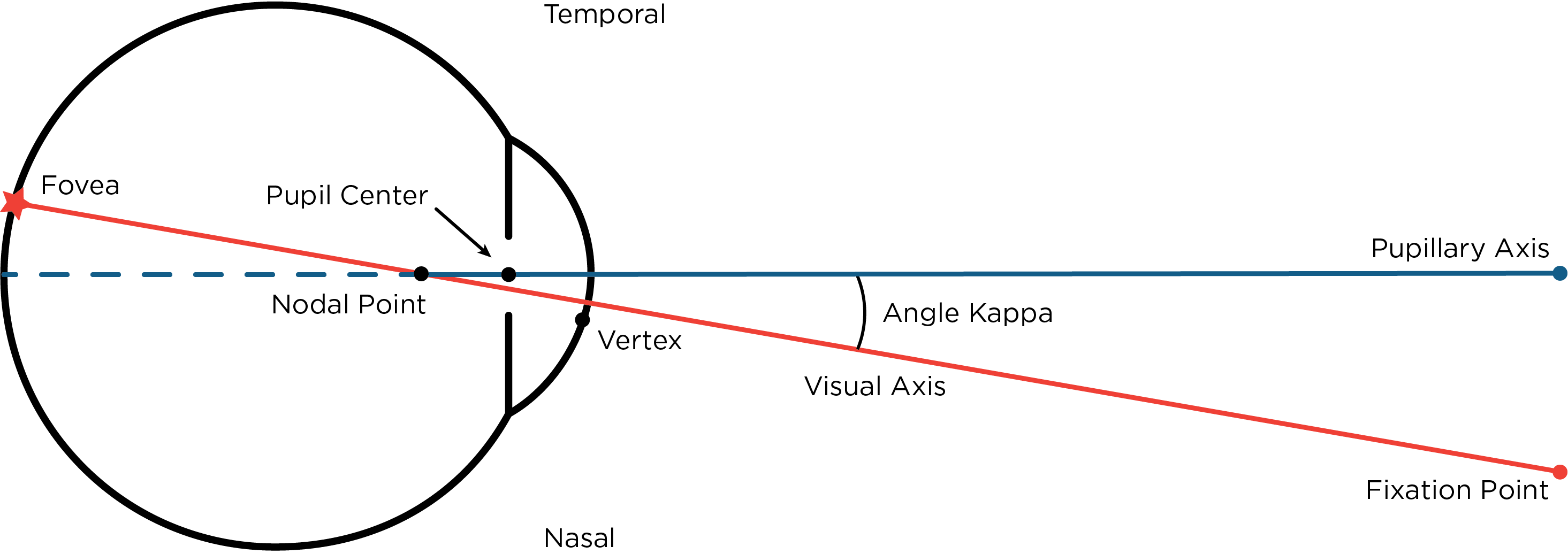
Angle kappa (Figure 3) is the angular distance between the visual axis (the line that connects the fovea to the fixation point) and the pupillary axis (line from the pupil center that is perpendicular to the cornea).Clinically this occurs because the corneal light reflex is displaced nasally from the pupillary center while the fovea is positioned temporally.2-4 Studies have shown that this causes most patients to have a slightly positive angle kappa. Similar to multifocal IOLs, when multifocal contact lens patients have small angle kappa, light can travel through the center of the lens to the fovea to provide balanced vision. However, when patients have a large angle kappa, a fovea centric light ray may pass through the edge of a multifocal zone and cause reduced vision and photic phenomena such as halos, glare and 3-D effects. 3-5 In a variety of studies, research has shown the following about angle kappa:
- A large angle kappa is more prevalent in hyperopic patients compared to myopic patients 2-4
- Gender is not related to angle kappa 2,6
- Angle kappa tends to be larger in left eyes compared to right eyes 2-5
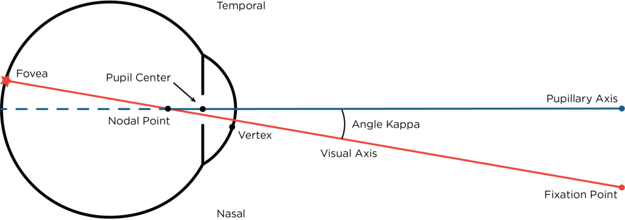
Figure 3. Angle Kappa
Conclusion
In conclusion, a misalignment between the multifocal optics and the patient’s visual axis can occur due to a variety or combination of factors. Regardless of the cause, this misalignment will alter the way the optics enter the eye and can ultimately lead to unhappy multifocal patients with unsuccessful lens fittings that should otherwise be a slam-dunk success. To help alleviate this issue, SpecialEyes is now offering the 54 Multifocal with OptiSync® Technology. This customization feature offsets (shifts) the multifocal optics from the center of the lens and targets alignment with the patient’s visual axis to improve your patient’s visual experience. To learn more about multifocal lenses with offset optics, be sure to check out the resources and studies below.
References
1 Hall LA, Young G, Wolffsohn JS, Riley C. “The influence of corneoscleral topography on soft contact lens fit.” Invest Ophthalmol Vis Sci. Aug; vol. 52, no. 9; 2011; pp. 6801-6806.
2 Park, Choul Yong; Sei Yeul Oh; and Roy S. Chuck. “Measurement of Angle Kappa and Centration in Refractive Surgery.” Current Opinion in Ophthalmology, vol. 23, no. 4; 2012; pp. 269–275.
3 Moshirfar, Majid; Ryann Hoggan; and Valliammai Muthappan. "Angle Kappa and Its Importance in Refractive Surgery." Oman Journal of Ophthalmology, vol. 6, no. 3; 2013; pp. 151–157.
4 Colin C.K. Chan and Brian S. Boxer Wachler. “Centration Analysis of Ablation Over the Coaxial Corneal Light Reflex for Hyperopic LASIK.” Journal of Refractive Surgery, vol. 22, no. 5; 2006; pp. 467–471.
5 Prakash, Gaurav; Amar Agarwal; et al. “Role of Angle Kappa in Patient Dissatisfaction With Refractive-Design Multifocal Intraocular Lenses.” Journal of Cataract Refractive Surgery, vol. 37, no. 9; 2011; pp. 1739–1740.
6 Hashemi H, Khabazkhoob M, Yazdani K, Mehravaran S, Jafarzadejpur E, Fotouhi A. “Distribution of angle kappa measurements with Orbscan II in a population-based survey.” Journal of Refractive Surgery, vol. 26, no. 12; 2010; pp. 966‒71.